CHOLANGIO TODAY: OUR VOICE
Breaks Silence. Spotlights What Works.
One mission — Enhance Today’s Patient Survival – today
By Steve Holmes — © 2025, Author and Copyright Holder
September 25th 2025
HER2 Overexpression Caused by Faulty ERBB2 Gene
HER2 overexpression is less common upstream — but in distal and gallbladder cancers, it’s far more frequent than most realise. Identifying it can open the door to new treatment options.
Podcast: Article Summary
Note: Some pronunciation errors occur.
Video: Article Highlights
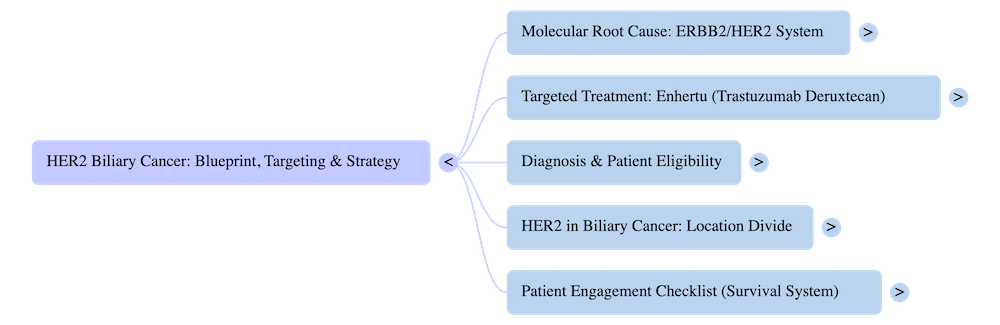
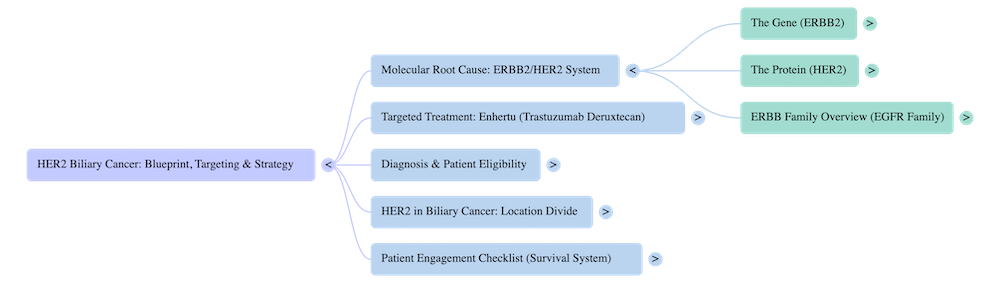
ERBB2 → HER2 → Enhertu
Gene → Protein → Targeted Treatment
Plain Language explanation:
What the ERBB2 gene normally does — and what happens when it fails.
The ERBB2 gene lives inside the cell nucleus, alongside more than 20,000 other genes. Its job is to control how much HER2 protein is made.
In healthy cells, ERBB2 sends instructions through mRNA, telling the cell’s factories to build just the right amount of HER2. These receptors sit on the cell surface and help regulate growth, repair, and survival.
But when the ERBB2 gene is damaged, its instructions become faulty. The growth signal gets stuck in **“go” mode.” This causes gene amplification — the cell makes far too many HER2 receptors.
The result is nonstop growth signals, pushing the cell into constant overdrive. This runaway growth is one of the key ways cancer begins.
Family-Friendly Insert — Cell City
Inside Cell City, the City Hall (nucleus) holds the master blueprint — the city plan. Each page is a different gene, and every page contains instructions to build something specific for the city.
The ERBB2 page holds the instructions for making HER2. When the city needs more HER2, ERBB2 calls in the city planners (mRNA) to copy the page. These copies are delivered to the construction factories (ribosomes), which build satellite receivers (HER2) and install them on the outer city wall (the cell membrane).
Like satellite dishes, these receivers pick up signals from outside the city and feed them inward. This helps the city grow and repair when it should — like an order being fulfilled.
Normally, ERBB2 acts as the growth switch, making sure the right number of receivers are built and pausing the signal once the job is done.
But when the ERBB2 page is damaged, the switch breaks. Messenger copies (mRNA) keep flying out nonstop. The construction factories work day and night, and soon the outer wall is crowded with satellites.
The crowded satellites keep pulling in nonstop “grow” signals, flooding the city with orders to expand. Without ERBB2’s ability to switch off or pause, the city spins into chaos.
This is how a single broken page in the blueprint can set Cell City on the path to cancer.
Decoder
- Cell → Cell City
- Nucleus → city’s control centre that stores DNA → City Hall
- DNA → the complete genetic blueprint → The City Plan
- Gene (ERBB2) → one section of DNA with instructions to build HER2 → A Page in the City Plan
- mRNA (Messenger) → copies the gene page and carries it out of the nucleus to the factories → The City Planner with the copied page
- Ribosome (Factory) → reads the mRNA copy and builds HER2 → The protein factories
- HER2 → a receptor made out of protein that sits on the outer cell membrane, receiving growth signals → The Satellite Receiver on the City surface
- ERBB2 → DNA snippet regulates HER2 production, pausing when enough are built → The Growth Switch
- Cellular Damage → when the cell is breached, its genes can be injured. If ERBB2 is hit, its DNA instructions become scrambled and hard to read. The growth switch breaks, leading to nonstop HER2 production → Runaway growth orders flooding Cell City.
Quick take
- What: Too many HER2 receptors on the cell surface
- Why it’s bad: Signals are amplified → cell gets nonstop “grow” commands
- Result: Uncontrolled growth — a key cancer driver
Plain Language explanation:
HER2 is a receptor on the outside of the cell. In healthy cells, the ERBB2 gene tightly controls how many HER2 receptors are made.
When ERBB2 goes faulty, it sends constant build orders. The cell’s surface becomes crowded with HER2.
More receptors = louder signals. Even normal growth cues now hit like a siren. Balance is lost. Growth overwhelms repair. That’s how tumors get momentum.
Family-Friendly Insert — Cell City
Picture Cell City’s wall lined with satellite dishes (HER2). City Hall (ERBB2) normally approves just enough.
When City Hall’s page is damaged and signals are jammed, factories pump out dishes nonstop. The city’s outer membrane wall is congested.
Now every passing message is picked up hundreds of times. The city is flooded with “Expand now!” orders — and it can’t switch them off.
Decoder
- HER2: A growth-signal receiver on the cell surface
- Overexpression: Too many HER2 receptors are made and positioned on the cell membrane
- Consequence: Normal signals become overamplified → runaway growth
Plain Language explanation:
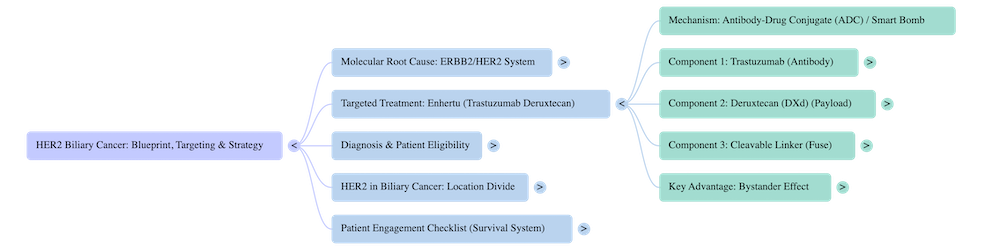
Enhertu – trastuzumab and deruxtecan is a type of antibody-drug conjugate (ADC).
Think of it as a smart bomb:
The antibody part (trastuzumab) is designed to find and stick to HER2 receptors on the cell surface. Once docked, it pulls a powerful chemotherapy payload (deruxtecan) directly into the cancer cell.
The chemo is released inside, damaging the cancer cell from within while leaving most healthy cells around it untouched.
This precision approach makes Enhertu especially powerful against cancers where HER2 is overproduced.
It targets the exact weak point created by the faulty ERBB2 gene.
Family-Friendly Insert — Cell City
In Cell City, the outer wall has become jammed with far too many satellite dishes (HER2 receptors).
These dishes are the problem — they keep flooding the city with nonstop “expand now!” messages.
Now imagine a special strike team arrives: Enhertu.
First, the team docks directly onto the satellite dishes that shouldn’t be there.
Then, once attached, they slip a demolition charge inside the wall.
Instead of blowing up the whole city, the charge goes off right where it’s needed — inside the faulty building.
This way, the strike team only takes down the dangerous parts of the city, while sparing most of the healthy structures.
Decoder
- Enhertu (trastuzumab deruxtecan): A targeted therapy called an antibody-drug conjugate.
- Antibody: The “homing device” that finds HER2 receptors.
- Drug payload (deruxtecan): The chemotherapy carried inside, released once inside the cancer cell.
- Why it works: Exploits HER2 overexpression by using the excess receptors as docking points, delivering chemo directly to cancer cells.

Plain Language explanation:
- HER2 levels are measured by a test called IHC (immunohistochemistry). The pathologist looks at how many cells have HER2 receptors on their surface, and how strong the staining is.
- HER2-positive (IHC 3+): More than 10% of tumor cells show strong, complete staining. This means lots of HER2 on the surface.
- HER2-low (IHC 1+ or 2+ without amplification): Tumor cells show faint or moderate staining, but not enough to be called HER2-positive. Still, Enhertu can sometimes target these.
- HER2-negative (IHC 0): No staining — Enhertu won’t work here.
- HER2 mutations (ERBB2 mutations on DNA tests): Sometimes genomic profiling shows mutations in the ERBB2 gene itself, which can also be treated with HER2-targeted drugs.
Family-Friendly Insert — Cell City
When city planners (pathologists) check the wall of Cell City, they count how many satellite dishes (HER2) are sitting there and how strong the signal looks.
- If lots of big dishes cover more than 10% of the wall → this is 3+ (HER2-positive).
- If only a few smaller dishes are scattered here and there → this is 1+ or 2+ (HER2-low).
- If the wall is bare, no dishes at all → this is 0 (HER2-negative).
- And sometimes, even if the dishes don’t look crowded, the blueprint (ERBB2 gene) itself has hidden errors — meaning HER2-targeted drugs may still work.
Decoder
Plain Language explanation:
Not every cancer shows the same cause. That’s why testing the tumor’s DNA is so important.
Genomic profiling looks at the cancer’s blueprint to see if ERBB2 is faulty or amplified.
If it is, doctors know the cancer is making too much HER2 — and that drugs like Enhertu may work.
Without testing, it’s guesswork. With testing, it’s precision: we match the right drug to the right patient at the right time.
Family-Friendly Insert — Cell City
Imagine trying to fix problems in Cell City without checking the blueprint. You’d be guessing which page was damaged.
Genomic profiling is like sending in expert city planners with magnifying glasses. They scan the blueprint, find the faulty ERBB2 page, and confirm why the city wall is overcrowded with dishes.
Now the repair team knows exactly where to target. Instead of trial and error, they bring in the precise strike team — Enhertu — to deal with the problem directly.
Decoder
- Genomic profiling: A test that reads a cancer’s DNA to find errors in genes.
- ERBB2 amplification: Too many copies of the ERBB2 gene, leading to excess HER2 receptors.
- Precision medicine: Using the test results to match the right targeted therapy to the patient.
⚖️ Patient flow recap:
- ERBB2 = the broken blueprint
- HER2 = the overproduced receptor on the cell surface
- Enhertu = the smart response that locks on and destroys HER2-positive cancer cells
- Genomic profiling = the patient’s advantage — the test that reveals the blueprint error so doctors can respond precisely
Plain Language explanation:
HER2 overexpression is not unique to one cancer. It can appear in several, often linked to aggressive growth:
- Breast cancer: 15–20% of cases are HER2-positive.
- Gastric / gastroesophageal cancer: Around 10–15%.
Bile duct and other GI cancers: A smaller but important subset.Why here? HER2 is a growth receptor. When it’s overproduced, tissues that rely on tightly controlled repair (like breast ducts or the stomach lining) become vulnerable to runaway expansion.
Family-Friendly Insert — Cell City
Overcrowded dishes can strike different cities in the body:
- In Breast City, the ducts are already busy hubs — too many dishes spark chaos.
- In Stomach City, rapid turnover of the lining makes it fertile ground for HER2 overload.
- Even in Bile Duct Cell Cities, a smaller neighborhood, HER2 overgrowth can drive aggressive tumors.
Decoder
- Breast cancer: HER2-positive in 15–20% of cases.
- Gastric / GEJ cancer: HER2-positive in ~10–15%.
- Other cancers (bile duct, lung, colon): smaller subgroups, but still important.
Plain Language explanation:
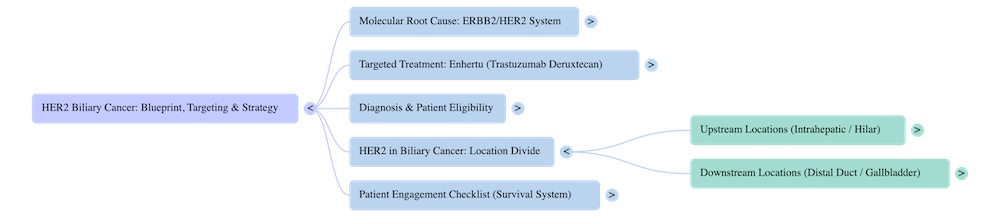
HER2 overexpression is not common in bile duct cancers, but it does appear in certain locations more than others:
- Intrahepatic (inside the liver): about 3–4%.
- Hilar / Perihilar (where the right and left ducts join at the liver hilum): around 3%.
- Distal (further down the bile duct, closer to the intestine): higher, about 15–20%.
- Gallbladder: can be 10–30% depending on the study.
Note: These numbers vary by study and testing method (IHC, amplification, sequencing). They’re not as well mapped as in breast or stomach cancers.
Why it matters: Knowing the location helps explain why HER2 testing is important. While less common in intrahepatic and hilar cases, HER2 can be a major driver in distal and gallbladder cancers — and that opens the door to targeted therapies like Enhertu.
Why the difference?
- Upstream (intrahepatic and hilar): lined by cholangiocytes — specialized duct cells built to withstand the most toxic bile in the body. Like heat shields on a rocket, they hold firm until they erode. When that happens, DNA takes heavy hits with double-strand breaks. Repair crews rush in but patch pages together the wrong way, leading to FGFR2 fusions and IDH1/2 mutations. HER2 amplification doesn’t appear here because these pathways are about structural mis-repairs, not signal overload.
- Downstream (distal ducts and gallbladder): bile here is diluted by water and bicarbonate added upstream, so it’s less toxic. The lining is columnar epithelium, more like the stomach and intestine. These cells are more flexible, higher turnover, less brittle. When they make mistakes, they don’t fuse blueprint pages — instead, they copy growth instructions too many times, leading to HER2 amplification.
Family-Friendly Insert – Cell City
- In Uptown (intrahepatic and hilar), the city walls are made of heat-shield tiles. They resist the bile storm every day. But once a tile erodes, there’s no second layer. The storm rushes in, blueprint pages tear, and repair crews patch them badly. Hybrid buildings rise — FGFR2 fusions, IDH1/2 errors — reshaping Uptown in dangerous ways.
- In Downtown (distal and gallbladder), the air is cooler, the bile storm weaker. The wall bricks here are ordinary — not as resistant, but they bend instead of shattering. When mistakes happen, it’s not torn pages — it’s too many satellite dishes. The city wall becomes crowded with HER2 receivers, flooding Downtown with nonstop “grow” messages.
Decoder
- Intrahepatic/Hilar: Cholangiocytes → resistant but brittle → bile toxicity causes DNA breaks → FGFR2 fusions, IDH1/2 mutations.
- Distal/Gallbladder: Columnar epithelium → flexible but less resistant → diluted bile, GI-like biology → HER2 amplification.
- Bile dilution: Upstream cholangiocytes secrete water + bicarbonate → bile becomes less concentrated downstream.
Pathway bias:
- Upstream → toxic bile → DNA breaks → fusions/mutations.
- Downstream → GI-like lining → signal amplification → HER2.
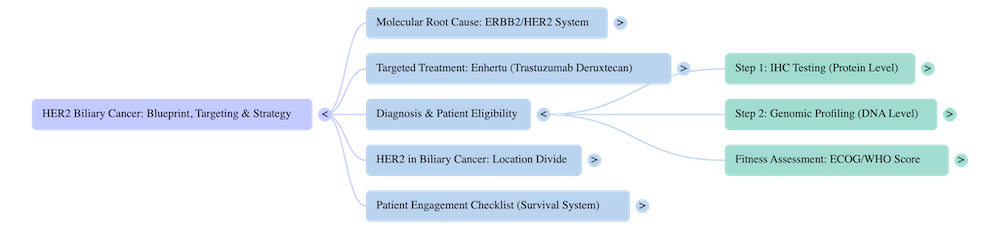
Plain Language
For treatments like Enhertu, the crucial test is IHC (immunohistochemistry).
This measures how much HER2 protein is present on the cell surface.
An IHC 3+ result confirms strong overexpression of the HER2 protein — a level that makes a patient eligible for HER2-targeted therapy such as Enhertu.
Genomic profiling can also be used; it looks deeper into the tumour’s DNA to identify other contributing errors or amplifications in key genes — like ERBB2 — that help explain why HER2 became overproduced in the first place.
In short: IHC is a fast and efficient test that finds the target; genomic profiling finds the cause.
Enhertu acts on the HER2 protein on the cell surface, not on the ERBB2 gene inside the nucleus.
Together, these tests give the full picture:
- IHC testing confirms whether the cell surface is overcrowded with HER2 receptors — the visible target.
- Genomic profiling reveals the fault in the blueprint — the ERBB2 gene that drives overproduction.
When both results align, clinicians know the target is visible and vulnerable — and Enhertu can dock precisely where it’s needed.
Family-Friendly Insert — Cell City
Imagine trying to fix problems in Cell City without checking the blueprint — you’d be guessing which page was damaged.
The IHC test is the city’s rapid-response scan, quickly spotting where the problem lies on the outer wall.
Genomic profiling is like sending in expert city planners with magnifying glasses. They study the blueprint, find the faulty ERBB2 page, and confirm why the city wall is overcrowded with satellite dishes.
That confirmation shows exactly where to target.
Instead of trial and error, the repair teams can now call in the precise strike team — Enhertu — to deal with the problem directly.
Decoder
- IHC (Immunohistochemistry): Shows how many HER2 satellite dishes are installed on the outer wall — used to confirm eligibility for Enhertu.
- Genomic profiling: Reads the city’s blueprint (DNA) to find faults like ERBB2 amplification or mutation.
- Why both matter: Genomic profiling explains why the error exists; IHC shows if the error built enough HER2 receptors to target.
- Enhertu target: HER2 protein on the cell surface — not the ERBB2 gene itself.
Plain Language
Genomic profiling is a test that reads the DNA of a tumor. It looks for errors in key genes — like ERBB2 — that can drive uncontrolled growth.
For HER2-positive cancers, this test confirms whether the cancer is being fuelled by too many HER2 receptors.
Family-Friendly Insert — Cell City
Imagine trying to fix problems in Cell City without checking the blueprint. You’d be guessing which page was damaged.
Genomic profiling is like sending in expert city planners with magnifying glasses. They scan the blueprint, find the faulty ERBB2 page, and confirm why the city wall is overcrowded with dishes.
Now the repair team knows exactly where to target. Instead of trial and error, they bring in the precise strike team — Enhertu — to deal with the problem directly.
Decoder
- Genomic profiling: Test that reads cancer’s DNA to find errors in genes.
- ERBB2 amplification: Too many copies of the ERBB2 gene, leading to excess HER2 receptors.
- Precision medicine: Matching the test results with the right targeted therapy.
Plain Language explanation:
Patients and families often ask the same key questions. Here are the answers — and prompts you can take to your oncologist.
FAQ
- Is HER2 inherited? No. HER2 overexpression is usually an acquired change in the tumor, not something passed down.
- Does HER2-low matter? Yes. Even with fewer receptors (IHC 1+ or 2+), new therapies like Enhertu can still work.
- Is HER2 the only test that matters? No. Genomic profiling may also show ERBB2 mutations or amplifications that guide treatment.
- Does HER2 mean worse prognosis? Not anymore. With targeted drugs like trastuzumab and Enhertu, HER2-positive cancers are far more treatable than they were 20 years ago.
Conversation Prompts
- “Can we confirm my HER2 status — and is it positive, low, or negative?”
- “Was my HER2 tested by IHC, ISH/FISH, or sequencing?”
- “If I am HER2-low, am I a candidate for Enhertu?”
- “What side effects should I watch for on HER2-targeted therapy?”
- “What’s the plan if my cancer stops responding — are there trials for HER2?”
Family-Friendly Insert — Cell City
Think of these questions as the city council meeting. You’re not just listening; you’re setting the agenda. By asking them, you steer the repair teams to the right problems.
In Closing
“When we see the cause, we can act.
When we understand the cause, we gain clarity.
Clarity reveals the path to a precise response.
This is the power of precision oncology, genomic profiling, and targeted medicines: giving oncologists sharper tools to identify what drives growth — and deliver treatments that strike at the source.”
— Steve Holmes
Donate
We exist because more people are being diagnosed with cholangiocarcinoma.
Once diagnosed, lived expertise leads those who are new.
That is what patient-led means:
- patient responsibility
- patient accountability
- a culture that is a survival system in itself — helping you help yourself.
But patient-led also means patient-funded — until others catch on.
We can’t wait.
We don’t have the luxury of time or “awareness.”
We execute what helps patients survive today.
We stand with you, shoulder to shoulder.
This is how we lead change.
This is how we outpace cholangio — now.
This is our difference. Our advantage.
If this work has helped you, join us.
Support the mission.
Resource Hub
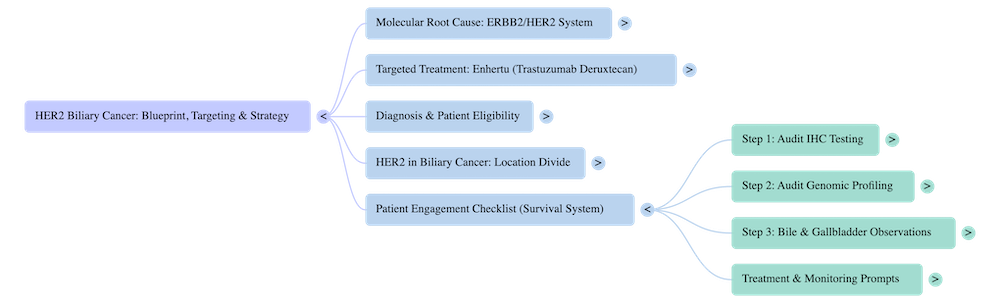
Patient Engagement Checklist
When facing HER2 biliary cancer, the right questions can make all the difference. This checklist gives patients and families a clear, practical guide to take into clinic, helping you stay confident, focused, and engaged in every decision.
- Download the Patient Engagement Checklist (PDF)
Patient Concept Expainer
- Download the Concept Explainer (For Patient) (PDF)
Official Product Website:
- product information
Enhertu – PBS website
Disclaimer
This information is shared patient to patient. It reflects Steve Holmes’ personal experience and deep engagement with the bile duct cancer journey. “While I’ve worked to ensure accuracy and clarity, this content is not medical advice. Always consult your healthcare team for guidance specific to your situation.”
Attribution
“© 2025 Steve Holmes. All rights reserved. Author and Copyright Holder: Steve Holmes. Published by the Cholangiocarcinoma Foundation Australia as part of the ‘Our Voice’ series.”
What Is Cholangio Today?
This is not awareness.
This is not care.
It is the expression and execution of
our patient-led culture —
a living survival system in itself.
It’s where we patients take the mic —
Not to tell stories.
To lead.
To shape systems.
To spotlight what works.
To share systems that deliver.
To extend response beyond care — through innovation.
We’re not here to raise awareness.
We’re here to raise survival.
This is not support.
This is how we win.
See a blind spot the system keeps missing?
Email: steve@cholangio.org