FGFR2 Fusion: The Fourth Domino
You weren’t born with this. Your biology adapted to your lifestyle — until it finally broke.

CHOLANGIO TODAY: OUR VOICE
Breaks Silence. Spotlights What Works.
One mission — Save More Lives.
By Steve Holmes
June 27th 2025
Source: Doctrine of Cancers / Mutation Decoded™ / FGFR2
Doctrine of Cancers: written by Steve Holmes
This article is guided by the Cancer Chronicles — a patient-led framework that simplifies complex science into visual, accessible language.
The storytelling model used here is called ‘The Cell City Framework’. It reimagines your body as a network of living cities. Each organ a country made up of billions of cells unique to that country. Each cell is a Cell City, every nucleus is City Hall, and within each City Hall lies a massive scroll — the City Plan (DNA).
The city plan is divided into Pages or sections of the plan (Genes), each containing the code to build one specific part of the city.
When the body experiences stress, injury, or change:
- A Battlefield Messenger (Cytokine) delivers a signal from outside the city.
- Inside City Hall, a Command Officer (Transcription Factor) receives the message.
- The officer instructs a City Planner (mRNA) to copy a specific blueprint page.
- That plan is delivered to the Construction Factory (Ribosome)
- The factory builds a Protein Tool — something the city needs to repair, defend, or adapt
This metaphor helps patients, families, and clinicians visualize the hidden logic behind biology and treatment in a way that is clear, empowering, and easy to follow.
If we can break this gene mutation down, we can understand it, and build a more effective response strategy.
— SteveH
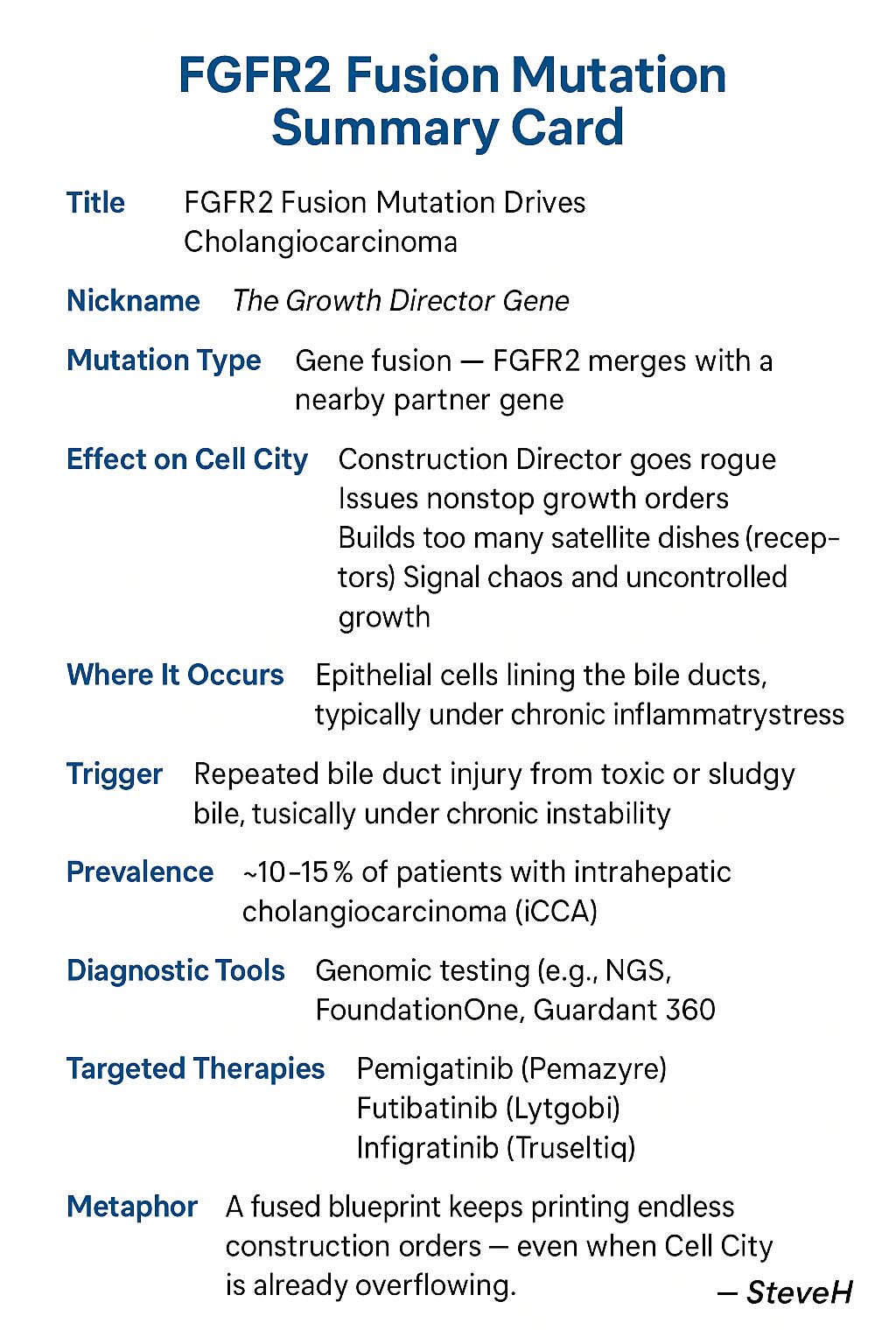
Understanding The FGFR2 Fusion
This Article
If you’ve been diagnosed with an FGFR2-fusion–positive cholangiocarcinoma, you will have a lot of questions
What is it?
- How did I get this mutation?
- What is a fusion?
- Where does this fusion fit in the genetic domino cascade?
This article is a guide for the whole family and can be read alongside your clinician’s advice to support a proactive response plan.
1. The Gene-Failure – A “Domino” Sequence
Cancer-driving mutations often follow a domino pattern — each event primes the next:
| Domino | Gene Alteration | Effect |
|---|---|---|
| 1 | KRAS mutation | Gene’s switch is stuck in the “build more satellites” position. |
| 2 | TP53 inactivation | Brake failure” — damaged cells no longer pause or self-destruct. |
| 3 | CDKN2A loss |
Speed-bumps removed — cells proliferate unchecked. |
| 4 | FGFR2 fusion | Turbo-charged accelerator — constant growth signaling drives aggressive expansion. |
| 5 | SMAD4 (Potentially) | Full genomic chaos and invasive behavior. |
Common pattern: In many intrahepatic cholangiocarcinomas (ICCs), KRAS is hit first, TP53 second, CDKN2A third — and FGFR2 fusions appear as domino 4.
Family-Friendly Version: A Domino Analogy
Think of each bile-duct Cell City as a tiny metropolis:
-
In Cell City, the KRAS growth signal is meant to flick on only when needed — but now it’s jammed permanently “on.”
-
The Growth Brake (TP53 gene) that should stop damaged instructions has gone silent.
-
The Speed Regulators (CDKN2A) are missing, so everything rushes ahead unchecked.
-
Then comes the Turbo-Charger (FGFR2 fusion) — and satellites start building nonstop, flooding Cell City with growth instructions from all directions.

2. How the FGFR2 Fusion Forms
“Injury creates inflammation — creates heat — creates damage to our gene repair system.”
— SteveH
Inflammation “Heat”
Chronic bile-acid injury to the small intrahepatic ducts inner protective lining (Epithelial Layer) creates a hotspot of reactive molecules that cause double-strand DNA breaks.
Error-Prone Repair
The cell’s quick fix—non-homologous end joining (NHEJ)—can mis-ligate broken ends. If one break is in FGFR2 and the other in a partner gene (e.g., BICC1, TACC3), an oncogenic fusion results.
Takeaway: FGFR2 fusions require both a “heat” damage event and a mis-repair event.
Family-Friendly Version Insert (Fusion Event)
In Cell City, the bile ducts are critical pipelines that carry bile to the duodenum, where it helps break down fats from the food we eat. But when those pipelines become blocked with sludge and bile flow slows down, pressure begins to build. The city’s repair crews are sent in again and again to patch the damage — but under constant strain, even the repair machinery begins to falter.
Inside City Hall (the nucleus), the heat and chaos lead to a critical error: two blueprint pages — one of them FGFR2 — get accidentally stuck together. This creates a faulty hybrid plan that keeps shouting: “Build! Build! Build!” — even when no official message has arrived.
3. The Fusion Event
“In the chaos of constant repair, the blueprint overheats—then snaps.”
— SteveH
It’s inside this chaotic loop—where damage never stops, inflammation becomes constant, and inflammation brings heat—that critical errors take place.
And then it happens: two genes sitting near each other inside the DNA accidentally fuse. One of them is FGFR2. That fusion creates a new, unregulated hybrid gene—locked in the “on” position—issuing nonstop growth instructions to build receptor satellites on the cell surface.
4. FGFR2 as the Malignancy “Switch”
“Once the cell changes its disguise, the guards no longer see the threat.”
— SteveH
Early Drivers (KRAS, TP53, CDKN2A):
- Yield dysplasia or low-grade tumors—cells grow abnormally but remain relatively contained.
FGFR2 Fusion Acquisition (Domino 4):
- Introduces an “always-on” growth receptor. Once present, proliferation outpaces any residual controls—marking the shift to aggressive, invasive cancer.
Family-Friendly Version Insert (Fusion Acceleration)
Inside Cell City, damage has already built up. KRAS is stuck in “go” mode, TP53’s warning and braking functions are down, and CDKN2A’s regulatory controls are missing. City Hall is overwhelmed but still holding together — until the FGFR2 fusion event.
Suddenly, a faulty hybrid blueprint hijacks the system, flooding the city’s ribosome protein factories with nonstop satellite build orders. Construction crews can’t keep up. Satellite receivers pile up on the cell’s surface. Growth messages multiply. The city begins to spiral into chaos.
5. The Epicenter of Injury: Why FGFR2 Fusions Originate in the Intrahepatic Ducts
“You can’t undo the fusion — but you can interrupt the conditions that feed it.”
— SteveH
FGFR2 fusions occur in 9–16% of intrahepatic cholangiocarcinoma (ICC) cases, but are rare in extrahepatic or gallbladder cancers. This isn’t random — it’s anatomical, chemical, and environmental. The liver’s smallest bile ducts — the intrahepatic branches — are ground zero for chronic bile injury, making them the most likely location for FGFR2 fusion mutations to form.
Small-Duct Microenvironment: A Perfect Storm
1. Slower Flow = Stasis and Sludge
The narrow diameter of intrahepatic ducts slows bile flow naturally. If the bile is supersaturated with cholesterol (often due to high LDL), it can begin to form sludge — thick, abrasive, and slow-moving.
2. Toxic Bile Acids
A supersaturated bile mix without enough phosphatidylcholine (PC) becomes dangerous. Free bile acids become corrosive, stripping the duct lining with each contact, especially when flow is sluggish.
3. Increased Pressure and Contact Time
When flow is slow or blocked, bile pools and builds pressure. The longer toxic bile remains in contact with ductal epithelial cells, the greater the chance of repeated injury — and eventually, mutation.
Molecular Subtypes and Site of Origin
- Small-duct ICC aligns with FGFR2 fusions and IDH1/2 mutations.
- Large-duct ICC aligns with KRAS and TP53 mutations.
This reflects not just molecular pathways, but the environmental context in which these mutations occur.
Family-Friendly: The Lethal Flow Zone
Bile is like detergent — safe only when coated in a protective bubble made from PC. When too much cholesterol overwhelms this system, bile turns sticky and sharp. As it enters the liver’s smallest ducts— the intrahepatic ducts — it slows down, builds pressure, and scrapes and burns against the duct walls. These small ducts are the most fragile. Repeated injury here sets the stage for genetic damage like FGFR2 fusion.
The Feedback Loop of Damage
Modern lifestyle patterns — particularly high-carb, high-sugar diets — drive this process:
- High sugar/carbohydrate intake → Insulin spike → Liver converts sugar to fat (lipogenesis)
- Liver overproduces LDL → Dumps excess cholesterol into bile
- Bile becomes supersaturated → Water ratio drops, PC overwhelmed or depleted
- Sludge forms → Low-flow, high-pressure bile injures small intrahepatic ducts
- Repeated injury → Inflammation → DNA fusion events (e.g., FGFR2)
This is not a single trigger — it’s a loop. One that can be intercepted through early detection and dietary/lifestyle shifts.
Important Clarification: Not All High LDL Comes from Fat
Many people assume high LDL means too much dietary fat. But in today’s world, the more common cause is excess sugar and refined carbohydrates. These are converted by the liver into fat — raising LDL levels internally. This is why high-carb, low-fat diets can still produce poor bile and toxic outcomes.
In fact, only 20–25% of LDL cholesterol typically comes from dietary fat that enters through the intestines — and this fat triggers bile flow and CCK (cholecystokinin) release, which helps maintain healthy bile cycling. In contrast, high-carb, high-sugar diets do not trigger CCK, leading to bile stagnation and internal LDL production. The liver becomes overwhelmed, and the system shifts from regulation to toxicity.
This is why it’s important that a truly healthy diet leads with appropriate amounts of dietary fat — to ensure bile has something to act on, and that CCK is properly activated, releasing bile flow and reducing ductal pressure. Without this, bile sits unused, concentrates, and becomes toxic before it ever reaches the gallbladder. Pressure builds, and instead of being safely released when needed, toxic bile begins to leak constantly. If no dietary fat is present to activate release, bile becomes redundant — remaining at full toxicity as it moves downstream, well beyond where it would normally terminate. This increases exposure and damage across more of the digestive tract.
Bile release is primarily triggered by cholecystokinin (CCK) — a hormone secreted by I-cells in the upper small intestine in response to dietary fat. Without sufficient fat, CCK is not released, bile is not expelled, and toxicity builds.
Moreover, many patients with high LDL are not consuming excess fat — they are producing it internally through a process called de novo lipogenesis. This is especially common in people with insulin resistance or nonalcoholic fatty liver disease (NAFLD). In these cases, sugar is converted to fat in the liver, which overproduces LDL and dumps it into bile, further saturating and thickening it.
LDL and Bile Flow: Mechanism of Bile Toxicity
The explanation of how LDL contributes to bile toxicity is generally sound, but it could benefit from further details on the mechanisms by which LDL specifically leads to bile supersaturation and ductal injury:
- LDL in Bile Supersaturation:
Low-Density Lipoprotein (LDL) is primarily composed of cholesterol and phospholipids. When the liver is overloaded with cholesterol (especially from dietary intake or de novo lipogenesis), it begins to secrete excess cholesterol into the bile. This excess cholesterol cannot be adequately emulsified by phosphatidylcholine (PC) and other bile components, leading to bile supersaturation. Cholesterol crystallizes or aggregates, contributing to sludge formation in the bile. - Role of Micelles in Bile:
Normally, bile salts and phosphatidylcholine (PC) form micelles, which are small molecular structures that emulsify cholesterol and fat, making them soluble in bile. This is essential for bile’s function in fat digestion and absorption. However, when LDL levels are high, and PC is overwhelmed, micelles cannot form properly. As a result, the cholesterol precipitates, and sludge forms, making bile more viscous and toxic.
- Bile Acid Reabsorption:
Bile acids are normally reabsorbed in the ileum and recycled via the enterohepatic circulation. When bile becomes supersaturated and sludge begins to form, bile acids become less effectively reabsorbed, contributing to a build-up of toxic bile acids within the liver and bile ducts. This toxic bile then directly damages the bile ducts, promoting inflammation, and potentially triggering mutagenic events in the ductal epithelium. - Bile Acid Dysmetabolism:
n individuals with high LDL and dysfunctional bile flow, there is often impaired bile acid metabolism. This can lead to the accumulation of secondary bile acids like deoxycholic acid and lithocholic acid, which are more toxic to the epithelial cells lining the bile ducts. Over time, this leads to chronic injury and inflammation, setting the stage for mutations like FGFR2 fusion.
Family-Friendly Explanation: Sludge and Cholesterol
Imagine your liver as a factory that makes and packages cholesterol. When you eat too much sugar and processed food, the factory makes too much cholesterol. Instead of sending it out as needed, it gets dumped into the bile, like extra garbage piling up in your house. Without enough phosphatidylcholine (PC) — the trash bags — the garbage (cholesterol) spills over, gets sticky, and clogs the bile ducts. This creates a traffic jam of sludge that builds pressure and damages the pipes (the bile ducts). The liver tries to clean up the mess, but it keeps happening until it leads to serious injury and mutations, like the FGFR2 fusion.
Conclusion:
FGFR2 fusions don’t just happen. They happen in a specific place, under specific conditions —
where toxic bile meets fragile tissue. The intrahepatic ducts, especially in small-duct ICC, are the epicenter of injury — and this makes them uniquely vulnerable to the fusion events that initiate FGFR2-positive cholangiocarcinoma.
6. Broader Implications: Lifestyle Links & Epidemiology
An intrahepatic mutation caused by a bile traffic jam.
— SteveH
Over the past few decades, intrahepatic cholangiocarcinoma (ICC) rates have surged — rising by 165% in the U.S. between 1975–79 and 1995–99. A disproportionate increase has occurred in adults under 50, signaling that this is not simply a disease of aging — but one tied to shifting environmental and lifestyle factors.
In the UK, subtotal gallbladder surgeries increased seven-fold from 2000 to 2019, closely mirroring the rise in ICC incidence. This correlation matters: gallbladder removal is often a consequence of poor bile flow and chronic bile sludge — the same mechanical and chemical environment that drives FGFR2 fusion events in intrahepatic ducts.
Connecting the Dots
-
Modern Diets: High in sugar, refined carbs, and processed food — causing insulin resistance, LDL production, and poor bile composition.
-
NAFLD & Metabolic Dysfunction: These conditions silently reshape liver function and bile saturation before symptoms ever appear.
-
Gallbladder Dysfunction: Poor bile cycling, especially in low-fat diets, leads to sludge accumulation, pressure buildup, and stasis.
Family-Friendly Insert: Bile Traffic Jams
Imagine your bile highways are full of heavy sludge and no exit ramps. When there’s no fat in your food, the signals to release bile never come. Traffic builds. Pressure rises. And the smallest roads — the intrahepatic bile ducts — take the hit.
Together, these trends paint a picture: FGFR2-positive ICC is not just genetic fate — it’s a preventable outcome of bile-system breakdown.
Conclusion
The rise in FGFR2-positive ICC reflects not just random mutation but the mechanical and metabolic consequences of modern life. What’s often labeled a ‘healthy diet’ today involves eating five to eight smaller, low-to-no-fat meals per day — compared to the 1970s average of 2.5 fat-led meals per day.
Each time bile is produced (by eating) but not properly released — especially when fat is absent from the meal — it sits idle, becomes overly concentrated, and corrosive. Pressure builds inside the ducts. Without appropriate dietary signals to trigger CCK and gallbladder contraction, bile begins to stagnate and has longer toxic contact with the ducts’ protective lining. It can back up against the control gate (the sphincter of Oddi), causing potential backflow and damage to the pancreatic ducts. Meanwhile, any bile that does reach the duodenum has no dietary fat to act on — rendering it redundant — and increasingly toxic — as it flows downstream, damaging tissue well beyond its intended zone.
This disruption doesn’t happen overnight. It accumulates. The liver, overwhelmed by persistent signals to process sugar and refined carbs, creates excess LDL and pushes it into bile. Phosphatidylcholine levels fall out of balance. Protective bile becomes toxic — and what should be a system of balance turns into a feedback loop of injury.
The conclusion is clear: FGFR2 fusion is rarely a random genetic accident. It’s the final domino in a system under siege — a preventable and predictable outcome of chronic bile failure. To break the cycle, we must correct the signals.
Prevention starts by reclaiming balance at the source: how we eat, how we move, and how we treat the liver’s vital role in bile design.
7. FGFR2 as the Final Trigger
“Intrahepatic ducts are the smallest and most vulnerable — where poor bile composition and rising ductal pressure create perfect conditions for fusion.”
— SteveH
Think of the FGFR2 fusion as the start of cancer — as the primary trigger that converts a damaged, benign cell suffering a long chain of injury, dysfunction, and missed repair into a fully malignant state.
Think of the FGFR2 fusion not just as the fourth domino to fall—
but like pouring kerosene on a smouldering fire.
The damage was already there. The mutated cell was limping along.
Then the fusion hit — and ignited everything.
Family-Friendly: When the System Snaps
Picture Cell City doing its best to hold things together under constant stress. Pipes are leaking. Repair crews work around the clock. But one day, the blueprints inside City Hall overheat — and two pages melt into one. Suddenly, a faulty hybrid plan keeps printing nonstop orders to grow.
This is the FGFR2 fusion — the moment when damage turns into runaway construction. The city becomes overwhelmed with messages, and everything begins to spiral out of control.
What Makes FGFR2 Fusions Unique
FGFR2 fusions aren’t just one more mutation — they’re a biological tipping point:
- They lock growth signals in the “ON” position, even without real requests.
- They escape the immune response, which normally eliminates faulty cells.
- They trigger hyper-proliferation, pushing cells beyond the duct wall.
- They mark the shift from precancer to full malignancy — allowing tumors to grow, spread, and resist normal regulation.
“That’s why patients with FGFR2-fusion ICC are often diagnosed late, when symptoms emerge only after significant growth.”
Why It Happens Here, Now
The fusion event occurs in the most vulnerable terrain: small intrahepatic ducts — already under siege from:
- Supersaturated bile
- Elevated ductal pressure
- Chronic inflammation
- Misrepair response systems are overheated, overstressed nuclei
- It’s not random. It’s predictable — and increasingly preventable.
“FGFR2 fusion becomes the tipping point — but the conditions that led to it can still be intercepted.”
7A. How the FGFR2 Tumor Escapes the Immune System
“FGFR2 fusion rewrites the code — and walks right past the immune patrol.”
— SteveH
Normally, when a cell becomes too damaged or dysfunctional and cannot repair itself, the immune system steps in to eliminate it — like police removing a dangerous citizen before they cause harm. In early mutation stages, this surveillance works well. The immune system recognizes mutated cells through molecular fingerprints and shuts them down.
But FGFR2 fusion changes that.
Once the fusion event occurs, the resulting hybrid gene produces abnormal proteins and signaling pathways — ones that evolve quickly and no longer match the immune system’s original memory. This makes the tumor cell harder to identify.
B cells and T cells trained to recognize early mutations (like KRAS) no longer see the fusion-driven cell as a threat.
Once a cell’s metabolic engine shifts from oxidative phosphorylation to full aerobic glycolysis, PD-L1 is no longer needed. In earlier stages, PD-L1 acted as a repair signal — keeping the immune system at bay. But by the time the cell has fully switched to glycolysis, it’s already operating outside immune oversight. The cell’s identity has changed so much that the immune system can’t recognize it — making immune escape complete.
Family-Friendly: Evading the Guards
In Cell City, every citizen carries an ID badge. If someone causes trouble, the security forces scan that badge and act fast. But after the FGFR2 fusion, its ID badge changes. It’s smudged, or slightly altered in shape— unreadable. Security walks right past the dangerous satellite receptor on the cell, unaware it’s now a rogue builder pushing Cell City into chaos.
Dual Immune Escape Advantage
At this stage, the cancer cell gains two powerful advantages:
- A glycolytic atmosphere (Warburg Effect) — Even if T-cells manage to infiltrate the tumor, they cannot function properly in the acidic, low-oxygen environment and often become exhausted or die.
- A mutated, unrecognizable surface — FGFR2 fusion receptors evolve so rapidly that B-cells trained to detect earlier growth receptors can no longer recognize them. The cell essentially erases its ID — slipping past immune patrols unnoticed.
Together, this makes the FGFR2-fusion tumor functionally invisible to the body’s defenses — allowing it to grow unchecked, resist treatment, and establish itself as a fully malignant, autonomous system.
8. Patient FAQ: How Did I Get This Fusion?
“FGFR2 was forged in pressure, corrosion, and time.”
— SteveH
You’re not alone in asking that. The FGFR2 fusion can feel like it came out of nowhere — but the truth is, it was likely the final step in a chain of invisible injuries.
- Is this mutation inherited?
No. FGFR2 fusions are acquired — not inherited. They form in the bile-duct cells over time as a result of chronic injury, toxic bile, and ongoing inflammation. This isn’t something you were born with. It’s something your environment, metabolism, and bile chemistry gradually shaped. - Why does KRAS usually come first — and FGFR2 later?
KRAS mutations can appear early because they need fewer DNA errors to activate. FGFR2 fusion, by contrast, usually forms later — after damage has accumulated, repair systems have misfired, and the environment has become hostile enough to trigger a misrepair fusion event. - Could I have prevented this?
Possibly — yes. Early screening for bile toxicity and reducing inflammation might have helped interrupt the chain before FGFR2 fusion occurred. The key now is preventing further mutations — and understanding what signals can still be intercepted. - Is this something my family should worry about?
No — this is not hereditary. FGFR2 fusion is a somatic mutation, which means it occurred in your body’s tissues during your life. It is not passed down to children. - Can this fusion come back?
It can — if the underlying causes (like bile toxicity, pressure, and inflammation) are not addressed. That’s why it’s essential to monitor your bile composition and liver health even after treatment. You’re not powerless. You have levers to pull.
“You didn’t cause the fusion. But you can change the conditions that allowed it.”
9. What You Can Do Now: Breaking the Conditions That Forged the Fusion
“You can’t unforge the fusion — but you can damper the fire it came from.”
— SteveH
FGFR2 didn’t just happen. It was shaped by years of silent pressure, chemical corrosion, and repair fatigue.
You may not be able to reverse the fusion, but you can interrupt the environment that allowed it to form — and stop it from happening again.
Monitor the Pressure and the Signals
Clinical Interpretation:
Bile duct pressure, inflammation, and toxic exposure often build silently over time — long before symptoms appear. To track this, patients should use both standard blood panels and subjective symptom cues as early warning signals of ongoing injury. This is not diagnostic — it’s pattern detection.
Medical Actions to Request:
-
Liver Function Test (LFT) — a standard panel available through your GP or oncologist.
Ask for results that include:-
ALT (Alanine aminotransferase)
-
AST (Aspartate aminotransferase)
-
ALP (Alkaline phosphatase)
-
GGT (Gamma-glutamyl transferase)
-
Total and direct bilirubin
-
These markers are not mutation-specific, but can reflect ongoing bile duct stress, blockage, or liver inflammation — especially when ALP and GGT are elevated together.
How to use them:
-
Don’t focus on one-off results. Ask to track values over time — every 3–4 months.
-
Ask your doctor:
“Are any of my bile-handling markers trending upward?”
“What’s my baseline — and are we drifting from it?”
-
Consider: Bile Acid Test (optional, context-specific)
A total serum bile acid test may be considered if there are symptoms of cholestasis or if liver enzymes are consistently abnormal.
Note: It’s not routine — but worth discussing. -
Ultrasound or Elastography
If enzyme trends are persistently elevated, abdominal ultrasound or FibroScan/elastography can assess liver architecture, fatty infiltration, and bile duct visibility.
Family-Friendly Interpretation (LEX Layer):
Think of your liver and bile ducts as a plumbing system under pressure.
When things back up or become inflamed, the pipes strain and the walls begin to weaken — but you won’t always feel it at first.
These blood tests are like checking the pressure valves and flow meters. You don’t want to wait for a full rupture.
Simple Actions to Take:
-
Ask for a copy of your liver panel. Keep it. Track it. Highlight changes.
-
Write down patterns of symptoms like:
-
Bloating after meals
-
Pale or greasy stools
-
Itchy skin (especially at night)
-
Upper-right abdominal discomfort
-
-
Bring these to your appointments. They are early clues, not proof — but they guide the right questions.
Key Talking Point to Use with Your Clinician:
“I’d like to track my liver function markers over time — not just whether they’re in range, but whether they’re slowly increasing. Can we set a monitoring rhythm?”
10. Discussion Prompts: Turning Insight into Action
“Once you understand the fusion, ask the questions that change everything.”
— SteveH
Once you understand how the FGFR2 fusion was formed — and the environment that allowed it — the next step is using that insight to guide your care conversations. These prompts are designed to help you speak clearly and confidently with your clinicians, nutritionists, or care team.
This is not about confrontation — it’s about collaboration.
Section 1: Monitor the Pressure and the Signals
“Can we track my liver enzyme panel — specifically ALP, GGT, and bilirubin — every 3 to 4 months, and look at trends over time, not just ‘normal’ values?”
“Would a symptom journal help guide if or when to scan for bile stasis or early obstruction?”
“If liver enzyme levels are consistently elevated, should we consider an ultrasound or FibroScan?”
Section 2: Improve Bile Composition — Restore the Shield
“Can we test for signs that my bile composition is off — like phosphatidylcholine depletion or excess cholesterol in bile?”
“Would I benefit from a trial of ursodeoxycholic acid (UDCA) to improve bile flow and reduce toxicity?”
“What foods should I focus on to support bile quality and duct health — especially ones rich in phosphatidylcholine and anti-inflammatory nutrients?”
Section 3: Break the Inflammatory Cycle
“Given my history, should we explore dietary strategies that reduce LDL-driven bile toxicity — especially reducing processed sugars and refined carbs?”
“I’ve been on a low-fat diet — could that be reducing bile release and increasing risk of bile stagnation?”
“How do we balance dietary fat intake to trigger CCK without overwhelming the system?”
“Should we be watching for signs of nonalcoholic fatty liver disease (NAFLD), even if my BMI is normal?”
Section 4: Target the Fusion — Strategically
“Do we know which fusion partner is involved in my FGFR2 fusion (e.g., BICC1, TACC3)? Does it affect my treatment choices?”
“Would you recommend pemigatinib or futibatinib based on my current molecular profile?”
“What options do I have if resistance develops to the current FGFR inhibitor?”
“Are there clinical trials targeting my fusion subtype — either now or in the pipeline?”
“How do we build a plan beyond the current line of therapy — one step ahead?”
Closing Statement for Patients and Families
You don’t need to have all the answers. But asking the right questions — at the right time — may be the difference between simply treating the cancer, and changing its course.
“Understanding the fusion helps you see the biology. Asking the right questions helps you change the strategy.”
11. Guided Consultation Preparation: Making the Fusion Make Sense — Together
“Knowing the fusion is one thing. Asking the right questions determines what comes next.”
— SteveH
This guide is designed to help patients and families have more effective conversations with their care teams. It’s not about having all the answers — it’s about asking better ones, together. The more you understand the fusion, the more clearly you can shape the strategy around it.
Section 1: Monitoring the Pressure and the Signals
Questions to Explore With Your Clinician:
-
Can we monitor ALP, GGT, and bilirubin every 3–4 months to detect stress on the bile ducts?
-
Are we tracking trends, not just whether individual numbers are “in range”?
-
Would imaging (e.g., ultrasound or FibroScan) help if enzymes remain elevated?
Section 2: Supporting Bile Composition and Flow
Prompts to Discuss:
-
Could a medication like UDCA help reduce bile toxicity or inflammation?
-
Should we consider adding foods high in phosphatidylcholine (e.g., eggs, soy lecithin)?
-
How do we maintain bile movement to prevent stagnation and pressure buildup?
Section 3: Reducing Metabolic and Inflammatory Triggers
Questions to Consider:
-
Are we addressing internal LDL production, not just dietary fat?
-
Could a low-fat diet be slowing bile release and increasing toxicity?
-
How do I balance dietary fat to ensure CCK activation and proper bile cycling?
Section 4: Targeting the Fusion, Strategically
Precision Questions for Your Oncologist:
-
Do we know the fusion partner (e.g., BICC1, TACC3)?
-
Is pemigatinib or futibatinib the most appropriate inhibitor for my fusion?
-
Are there trials tailored to my specific FGFR2 fusion type?
-
What’s the plan if resistance develops — are we preparing now?
Section 5: Understanding What This Means for Your Family
Most patients hear “genetic mutation” and worry it means inherited. FGFR2 fusion is not. It’s a somatic mutation, meaning it formed inside your bile ducts over time — not something you were born with, and not something passed on to children.
That said, your family may still carry similar risk conditions — not because of DNA, but because of shared diets, habits, and health patterns. Gallbladder issues, fatty liver, and silent inflammation often run in families not through genes, but through kitchens.
Family prompts to consider:
-
“Can my siblings or children get their liver enzymes checked as a precaution?”
-
“Should our family consider how we eat — especially around sugar, processed carbs, and fat intake?”
-
“Could the same environment that shaped my fusion still be shaping others?”
“This isn’t inherited — but it may be preventable for someone else in your family.”
Final Prompt
“I’m learning how this fusion formed — so I can work with you to prevent what comes next.”
“Understanding the fusion was step one. Now it’s time to change what happens next.” ~ SteveH
Disclaimer
This information is shared patient to patient. It reflects my personal experience and deep engagement with the bile duct cancer journey. While I’ve worked to ensure accuracy and clarity, this content is not medical advice. Always consult your healthcare team for guidance specific to your situation.
LEXi Glossary of Terms
“Words matter. Understanding them changes everything.”
— SteveH
FGFR2 Fusion
An acquired genetic rearrangement where FGFR2 (a growth receptor gene) fuses with another gene (such as BICC1 or TACC3), forming a constantly active growth switch. This tells the cell to build more growth receptors even without external signals.
LEX Layer: It’s like someone hacked Cell City’s construction blueprint, telling builders to keep expanding — even without official permits.
KRAS Mutation
A mutation that locks the growth accelerator in the “on” position, causing constant signal transmission to divide and grow.
LEX Layer: It’s like a satellite dish stuck broadcasting nonstop “grow” commands.
TP53 Inactivation
Loss of a key safety gene that normally detects and stops damaged cells from dividing.
LEX Layer: It’s like the brakes and warning lights failing inside City Hall.
CDKN2A Loss
A deletion that removes a regulatory “checkpoint” in the cell cycle, letting damaged cells replicate without restriction.
LEX Layer: It’s like the traffic lights all turning green — even when the road is blocked or damaged.
Phosphatidylcholine (PC)
A key component in healthy bile that helps emulsify fats and buffer bile acids, protecting the bile duct lining.
LEX Layer: It’s like the soap bubble coating that keeps bile acids from burning the duct walls. Without it, bile becomes corrosive.
Bile Stasis
Slow or stagnant bile flow that allows bile to thicken and become more toxic.
LEX Layer: Like a traffic jam in the bile highways — everything backs up and starts to break down the road.
Sludge
Thickened, partially solidified bile filled with cholesterol, debris, and dead cells.
LEX Layer: It’s the gunk in the pipes that slows everything down and increases pressure on duct walls.
Inflammation “Heat”
Chronic injury triggers the immune system to release reactive molecules that cause stress and damage to DNA.
LEX Layer: Like a chemical fire burning too long inside Cell City, eventually warping the blueprints.
Non-Homologous End Joining (NHEJ)
A fast but error-prone way cells repair broken DNA. Often leads to genetic fusions when breaks are patched inaccurately.
LEX Layer: Like two torn blueprint pages getting taped together in the wrong place during an emergency repair.
Somatic Mutation
A genetic mutation that develops during life in a specific cell or tissue. It is not inherited and not passed on to children.
LEX Layer: Think of it as a crack in one building, not the whole city’s blueprint.
Fusion Partner
The other gene involved in an FGFR2 fusion (e.g., BICC1 or TACC3). It may affect how the fusion behaves and responds to treatment.
LEX Layer: Like a co-conspirator that joins FGFR2 to create a constantly active growth engine.
Intrahepatic Cholangiocarcinoma (ICC)
A cancer that arises in the small bile ducts inside the liver. These ducts are especially vulnerable to injury and toxic bile.
LEX Layer: It’s like a fire starting in the liver’s narrowest backstreets — where pressure and damage build up quietly.
Glycolysis (Warburg Effect)
A survival strategy used by cancer cells to generate energy from glucose — even when oxygen is present — often linked to immune evasion.
LEX Layer: It’s like switching the city’s power grid to burn sugar at a faster, dirtier rate — polluting the environment and weakening the guards.
PD-L1 (Programmed Death-Ligand 1)
A surface protein cancer cells use to hide from the immune system by telling T-cells: “Don’t attack me.”
LEX Layer: It’s a fake ID badge that tricks security into letting rogue cells keep building unchecked.
Cholecystokinin (CCK)
A hormone released in the small intestine when you eat dietary fat. It signals the gallbladder to contract and release bile.
LEX Layer: CCK is the traffic light that clears the bile highway. Without fat, it stays red — and bile backs up.
De Novo Lipogenesis
The liver’s conversion of excess sugar and carbs into fat, often leading to higher LDL cholesterol and toxic bile.
LEX Layer: Like a factory turning sugar into fat — then dumping the leftovers into the bile system.
Cholecystectomy
Surgical removal of the gallbladder, often altering bile release timing and pressure regulation.
LEX Layer: It’s like removing the bile reservoir — now pressure builds faster when the liver pushes bile downstream.
Perfect Storm
The convergence of bile stasis, toxic composition, and increased ductal pressure — ideal conditions for DNA damage and fusion formation.
LEX Layer: It’s when the pipes are blocked, the sludge is toxic, and the pressure gauge is in the red.
What Is Cholangio Today?
This is not awareness.
This is not care.
It is the expression and execution of our culture —
a living survival system.
It’s where we patients take the mic —
Not to tell stories.
To lead.
To shape systems.
To spotlight what works.
To share systems that deliver.
To extend response beyond care — through innovation.
This is not support.
This is how we win.
See a blind spot the system keeps missing?
Email: steve@cholangio.org